

Background:
Leukemia relapse after allogeneic hematopoietic cell transplantation (alloHCT) has been associated with loss of heterozygosity of class II HLA, suggesting that T cells targeting leukemia via class II interactions may be critical for graft-vs-leukemia (GvL) effects and protection from relapse (Zeiser & Vago, 2019). Therefore, we aimed to determine whether the number of predicted class-II restricted minor histocompatibility antigens (mHAs) in alloHCT recipients associates with clinical outcome. Specifically, we investigated: (1) if the number of mHAs expressed on leukemia and bone marrow cells (GvL mHAs) is correlated with incidence of leukemia relapse, and/or (2) if mHAs expressed on acute graft versus host disease (GvHD) target organs (GvH mHAs) correlated with incidence of GvHD. We expected increased GvL mHAs to be associated with increased survival, and increased GvH mHAs to be associated with increased incidence of GvHD.
Methods:
The study population was derived from donor-recipient alloHCT pairs (DRPs) treated for Acute Myeloid Leukemia (AML), Acute Lymphocytic Leukemia (ALL), and Myelodysplastic Syndrome (MDS) from the CIBMTR and previously analyzed in DISCOVeRY-BMT. To predict HLA class II restricted mHAs in alloHCT recipients, we translated nonsynonymous single nucleotide variants present in each recipient, but absent in their respective donor, into all possible peptides 15-24 amino acids long. We used netMHCIIpan to score these peptides and select those most likely to be presented (Reynisson et al., 2020). Predicted mHAs highly expressed in skin, hepatobiliary, and bowel tissues were classified as GvH mHAs, and those highly expressed highly in, testis, and bone marrow were classified as GvL mHAs. The impact of mHA on disease related mortality (DRM), leukemia free survival (LFS), disease relapse and death due to GVHD were assessed with competing risk models. We next determined whether knowledge of the number of GvL and GvH mHAs improves the ability of models to predict clinical outcome. We fit optimal logistic regression models (elastic net regularization with Monte Carlo cross validation) to predict GvHD mortality and relapse mortality at 1 year after alloHCT using: (1) clinical data only, and (2) both clinical data and number of GvH/GvL mHAs. Lastly, using the same regularization and cross-validation procedures as above, we determined which variables contributed most to the Cox regression models of overall survival.
Results:
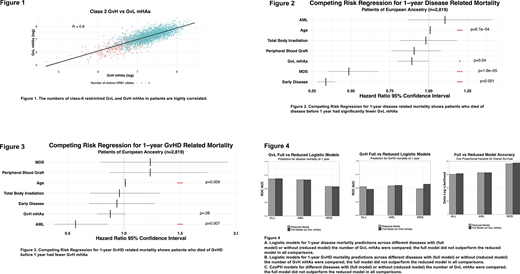
The number of GvL-restricted and GvH-restricted class-II mHAs were significantly correlated (Figure 1). Patients who died of disease before 1 year after alloHCT had significantly fewer GvL mHAs when controlling for covariates (HR=.89, 95% CI .89, .99, P= 0.04) (Figure 2). There was no association between GvL mHAs and LFS or relapse. Surprisingly, death due to GvHD by 1 year after alloHCT was lower for recipients with more GvL mHAs (HR=.88, 95% CI= .76, 1.01 , P=.08) (Figure 3), however, because GvH and GvL mHAs are highly correlated, we believe this reflects better overall survival associated with increased GvL mHAs. Neither the predictive models that included the number of GvH/GvL mHAs nor the Cox regression models fitted with GvL mHA numbers performed better than models trained on clinical data alone (Figure 4).
Conclusions:
GvL mHAs were inversely associated with DRM at 1-year post-alloHCT as expected. Contrary to our hypothesis, the number of GvH mHAs was inversely associated with GvHD mortality at 1 year. This may reflect better overall survival associated with increased GvL mHAs, as GvH and GvL mHAs are highly correlated. The potential association between class-II mHAs and DRM warrant further investigation and validation. If validated, this supports the development of class-II mHA targeted immunotherapies.
Pasquini:Bristol Myers Squibb: Consultancy; BMS: Membership on an entity's Board of Directors or advisory committees, Research Funding; Amgen: Other; Novartis: Research Funding; Kite: Research Funding. Armistead:GeneCentric: Consultancy; Cell Microsystems: Patents & Royalties: Patent application U.S. 16/347,104 "Automated collection of a specified number of cells". Vincent:GeneCentric Therapeutics: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal